
Steroid Side Effects – Cardiovascular System
The heart can suffer serious damage as a result of the use of anabolic/androgenic steroids in dosages that go beyond the recommended (therapeutic) levels. It is possible to detect this by observing certain features such as abnormal alterations in serum cholesterol, ventricular wall thickening, increased blood pressure, and changes in vascular reactivity. Although these drugs are safe when applied immediately. It is even extremely unlikely that a perfectly healthy person will have a heart attack due to one steroid cycle.
The same applies to cases of stroke because it is also very rare. However, when these drugs are used for long periods they would negatively affect the cardio system with time being given for their build-up hence leading to early deaths from cardiac arrests or strokes which are also frequent risks posed by prolonged abuse of steroids. Therefore, one should understand well how the cardiovascular system is affected by anabolic/androgenic steroids through some critical channels.
Cholesterol/Lipids
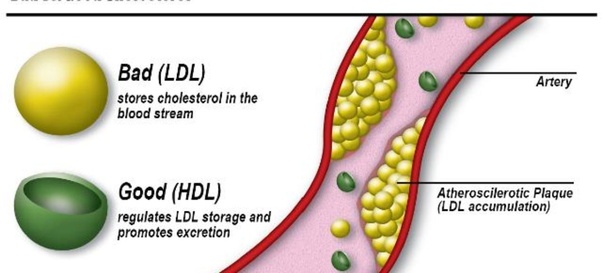
Anabolic/androgenic steroids have been shown to reduce HDL (good) cholesterol whilst increasing LDL (bad) cholesterol values when they are abused. Comparing HDL and LDL cholesterol figures gives an overall idea of the artery walls’ condition concerning plaque build-up between anti-atherogenic and atherogenic factors respectively.
The overall scenario in steroid use is a decrease in HDL levels, often combined with normal or higher LDL levels. There may as well be an increase in triglycerides. It’s really bad in every way. I’d like to note right here that the total cholesterol count sometimes does not change considerably. Thus, total cholesterol might misrepresent undamaged lipid health. It cannot be but this one thing there is always a reduction of the ratio of underlying HDL/LDL.
When steroids’ intake is interrupted, this relation should return to order though plague blockages within arteries become more permanent. If such disruptive shifts are compounded by long-term use of steroidal compounds, it may result in severe damage to the cardiovascular system. With time, plaque deposits can begin narrowing and clogging arteries.
HDL Lowering Is Most Pronounced With Anabolic Steroids
The androgenic effects of these drugs stimulate hepatic lipase that breaks down good or HDL cholesterol from your liver. The more hepatic lipase present in your body, the faster (anti-atherogenic) HDL cholesterol particles are eliminated from circulation and their concentrations fall hence. The magnitude of this effect appears to be quite large at even moderate supratherapeutic doses for example.
For instance, a decrease in HDL cholesterol of 21% was observed in tests conducted with testosterone cypionate at 300 mg per week. However, increasing this dose to 600 mg had no significant added impact, showing that the HDL suppression level of such a steroid is rather low.
Orally administered steroids, particularly c-17 alpha alkylated ones, are potent stimulators of hepatic lipase and suppressors of HDL levels. This is because of their concentration and metabolism by the first-pass effect through the liver.
Therefore drugs like stanozolol can be milder than testosterone concerning androgenic side effects while they cannot when it comes to cardiovascular strain. This study therefore brings out very clearly how different these two drugs are as it compares the effects of a weekly injection of 200mg testosterone enanthate with only 6mg daily oral doses of stanozolol.
Within just six weeks, an average drop in HDL cholesterol levels by 33% and HDL-2 subfraction by up to 71% were recorded with stanozolol at 6mg/day. Only a minor cutback – only about nine percent took place within the testosterone group on its own which resulted from a decrease in HDL cholesterol (mainly the HDL-3 subfraction).
Stanozol, however, saw an increase of 29% in levels of LDL cholesterol while testosterone showed a drop of 16%. Esterified injectable steroids are generally less stressful to the cardiovascular system than oral agents. Moreover, it is important to note that estrogens can favorably impact cholesterol profiles. Therefore, the aromatization of testosterone to estradiol may prevent an acute alteration in serum cholesterol.
In this study, lipid changes caused by 280 mg of testosterone enanthate weekly were examined and compared against those caused by the same dose when accompanied by testolactone which is an aromatase inhibitor. Additionally, a third group took methyltestosterone at a dosage of 20 mg daily to investigate what difference would be inflicted by oral alkylated steroids. However, there was no significant decrease in HDL values throughout this study for subjects using only testosterone enanthate (Group I).
Nevertheless, within four weeks following commencement, HDL dropped from an average of 25%, after using an aromatase inhibitor with testosterone (Group II) for twelve weeks. The most pronounced fall (35%) occurred within four weeks among those taking methyltestosterone (Group III);
This group also found out that there was an unfavorable increase in LDL cholesterol levels. The issue of estrogen maintenance may likely have a potentially positive effect on cholesterol values, which should also be taken into consideration when it comes to health risks. At first, one might like to question if or not estrogen maintenance drugs are really necessary for any given situation. Are there observable side effects or is their use a preventive step and maybe a waste of time?
Conversely, a patient who is put on the right maintenance drug will experience an improvement in his or her cholesterol levels. Some patients taking tamoxifen citrate (which is an estrogen receptor antagonist) do not see antiestrogenic effects on serum lipids, and have higher HDL levels; others with aromatase inhibitors instead prefer tamoxifen because they believe that it helps against estrogenic side effects when they use steroids for longer intervals and worry about the total sum of cardiovascular problems these could cause them eventually.
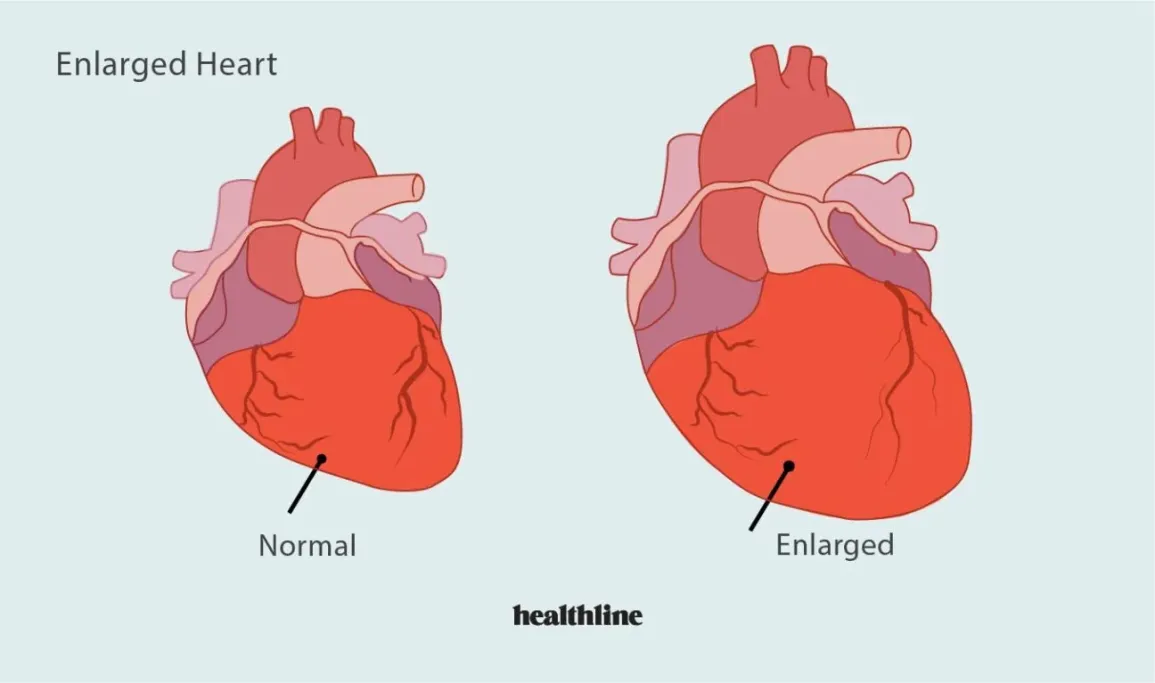
Enlarged Heart
A human heart is a muscle. It has functional androgen receptors and can grow in response to male hormone steroids. This accounts for the fact that men have on average larger hearts than women. Exercise is also a strong determinant of the size of hearts. This type of exercise leads to an increase in the thickness of the ventricular wall, which usually does not come with equal internal cavity expansion; it is referred to as concentric remodeling.
Endurance (aerobic) athletes, on the other hand, tend to increase heart size via expansion of the internal cavity, without significant thickening of the ventricles (eccentric remodeling). In either case, diastolic function tends to remain normal in the athletic heart. The heart muscle is alive too. After prolonged training is stopped among conditioned athletes, wall thickening and cavity expansion tend to decrease.
Heart Muscle Damage
In some cases, abuse of anabolic/androgenic steroid use is thought to directly damage cardiac muscles. These studies showed reduced contractility, increased fragility as well as decreased mitochondrial activity in cultures exposed directly to AAS thereby supporting a possible direct toxic effect on heart muscle cells.
Additionally, there are several case reports of myocardial fibrosis (such as scar tissues developing in the heart), myocarditis (which is an inflammation of heart muscles), cardiac steatosis (the accumulation of triglycerides within the heart cells), and myocardial necrosis (death of heart muscle fibers) in long term users of steroids. There is a clear correlation between drug use and cardiac diseases, however, this relationship cannot be proven because cardiac pathologies develop slowly and other factors like diet, exercise, lifestyle, genetics, etc also play a role. Individuals must take caution about long-term steroid abuse possibly causing damage to their hearts.
Blood Pressure
Anabolic/androgenic steroids could lead to high blood pressure. Studies on weightlifters using these substances at excessive dosages showed an increase in both systolic and diastolic pressures. Another research work found that the average blood pressure among a group of steroid users was 140/85, compared to 125/80 for controls who were lifting weights but did not take any drugs.
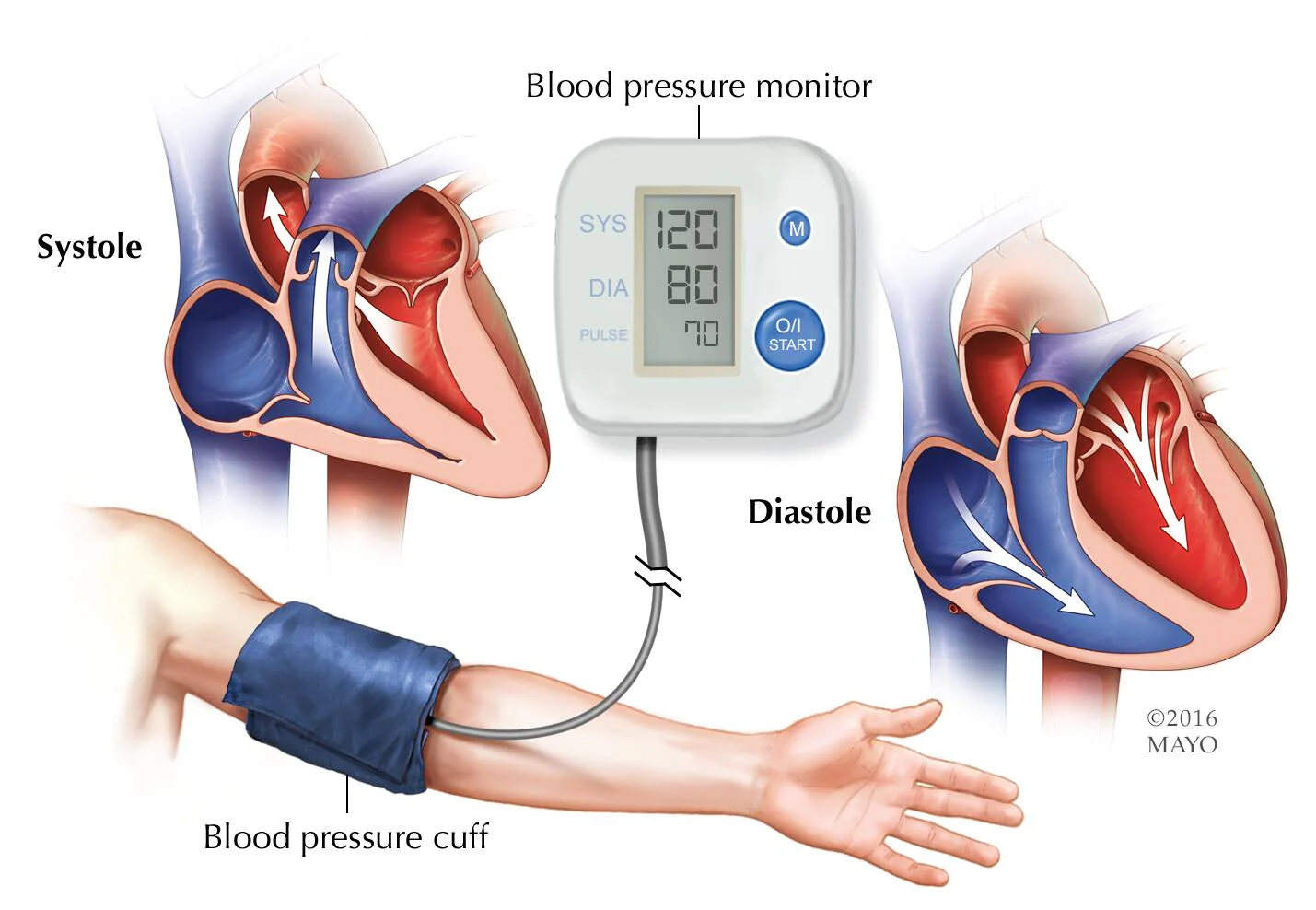
Steroid users typically show hypertension, which is regularly known as high blood pressure at or above 140/90 for either systolic or diastolic measures. However, the related increase in its levels is usually slight. Various factors like increased water retention, increased vascular stiffness, and increased hematocrit can raise blood pressure. Most powerful effects on blood pressure are usually produced by steroids with aromatizing or highly estrogenic activities whereas they cannot be ruled out for non-estrogenic anabolic/androgenic steroids. After stopping using anabolic/androgenic steroids, the blood pressure usually returns to normal.
Write a comment