

An Introduction to Testosterone
Anabolic steroids are a class of drugs that contain an artificially produced hormone testosterone, or any other compound derived from this hormone. To fully understand how anabolic steroids function one must first know the basic working principle of testosterone.
Testosterone is the key male sex hormone. It is secreted by the Leydig’s cells in varying quantities throughout the life of an individual. During puberty, when there is a higher output of testosterone, its effects become most apparent as there will be dramatic physiological transformations in the body of males such as deepened voice, growth of body and facial hair, increased sebaceous gland secretion, development of sexual organs, maturing sperm, and high sexual desire.
In fact, without significant amounts of testosterone, normal functioning cannot take place in the male reproductive system. Androgenic properties refer to all these effects hence they can also be termed masculinizing. Also increase in the production of testosterone will bring about anabolic changes well known to involve higher protein synthesis rates causing muscle growth.
Different levels of testosterone in the body are responsible for men having more muscle mass compared to women. For instance, a mature male will produce between 2.5 and 11 mg each day while females make only about a quarter of this amount. Conversely, estrogen is the most dominant sex hormone in women and it has different effects on the body. Women with less androgen and more estrogen will tend to have higher amounts of body fat, lesser masses of muscle tissue, be smaller in size, and become at risk of osteoporosis as they age. The exact mechanism by which these changes occur due to testosterone is quite complicated.
When not bound to anything, the molecules can move around easily in the bloodstream until they come into contact with their target cells. This includes skeletal muscle cells as well as skin, scalp kidney bone central nervous system prostate tissues among others. The cellular target interacts with testosterone causing its effect; thus it only affects those cells having appropriate hormone receptors (mainly androgen receptors). In this case, every specific type of hormone is activated by a specific kind of receptor like a lock key system where each key goes into a particular lock only.
In the course of this interaction, the testosterone molecule will bind to the intracellular receptor (located in cytosol not on the surface of the membrane) and form a new “receptor complex”. This hormone-receptor complex then moves into the nucleus and binds to a specific part of its DNA called the hormone response element.
Transcription of some genes will be activated for example, in muscle cells, skeletal muscle cells through gene transcription would ultimately lead to increased synthesis of actin and myosin which are the two main contractile proteins involved in muscular growth. Additionally, androgens may increase carbohydrate storage in muscle tissue.
Upon completion of this messaging process, the complex is released thus disassociation between receptor and hormone takes place. Both can now move back to the cytosol for further activities. The testosterone molecule can also diffuse back into circulation to interact with other cells. The entire cycle from the initial binding of a hormone by a receptor through migration as a receptor-hormone complex into nuclear localization signals (nls), transcriptional activity ending with separation and release back into the cytoplasm is a slow process requiring several hours but not minutes. For example, studies using nandrolone given once intramuscularly have shown that it is measured to be 4 to 6 hours before free androgen receptors migrate back to the cytosol after activation.
It is also suggested that this cycle includes the splitting and formation of new androgen receptors once returned to the cytosol, a possible explanation for the many observations that androgens are integral in the formation of their receptor sites. In the kidneys, this same process works to allow androgens to augment erythropoiesis (red blood cell production). It is this effect that leads to an increase in red blood cell concentrations, and possibly increased oxygen transport capacity, during anabolic/androgenic steroid therapy.
Many athletes mistakenly assume that oxymetholone and boldenone are unique in this ability, due to specific uses or mentions of this effect in drug literature. Stimulation of erythropoiesis occurs with nearly all anabolic/androgenic steroids, as this effect is simply tied to the activation of the androgen receptor in kidney cells.
The only real exceptions might be compounds such as dihydrotestosterone and some of its derivatives, 4 which are rapidly broken down upon interaction with the 3alpha hydroxysteroid dehydrogenase enzymes (kidney tissue has a similar enzyme distribution to muscle tissue, see “anabolic/androgenic dissociation” section), and therefore display low activity in these tissues.
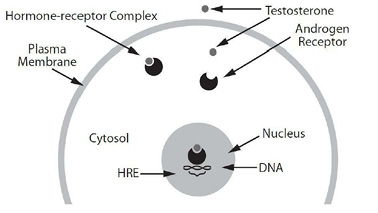
CELLULAR DIAGRAM: Testosterone freely diffuses through the plasma membrane and binds with an intracellular androgen receptor.
The hormone-receptor complex then enters the cell nucleus to bind with a specific segment of DNA (the Hormone Response Element), activating the transcription of specific genes.
Write a comment