

The Most Effective Growth Hormone Protocol for Fat Loss
Growth Hormone (GH) is an agent that effectively mobilizes fat. Researchers have been aware of its potential since the 1920s, when early animal trials showed that animals treated with hormones were consistently leaner, than those not treated. It wasn't until 1945 that scientists first extracted GH from the gland and began to isolate the effects of fat mobilization specific to this particular polypeptide.
What is Lipolysis? – Explanation
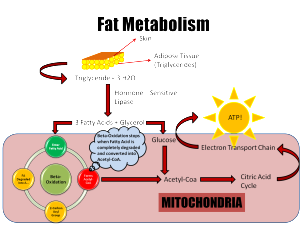
Lipolysis is a process that provides the body with energy by breaking down stored fat into fatty acids and glycerol. These molecules are then released into the bloodstream, for conversion into ATP, which is used for energy production. While it's worth noting the distinctions between mobilization and oxidation, delving into an exploration of lipolysis is beyond the scope of this article.
The Stress Hormone / Relationship of GH and Fasting
GH, a hormone associated with stress is naturally secreted in amounts during periods of fasting and exercise. The postabsorptive phase, which typically begins around six hours after eating, is characterized by the body's efforts to supply, convert and preserve fuel sources. During this phase there is an increase in the secretion rate of GH that can last for 48-72 hours. The amount of GH secreted correlates with pulse strength while the frequency and trough levels between pulses remain relatively constant. Interestingly GH is the hormone that increases during fasting while catabolic hormones such as glucagon, cortisol and epinephrine also experience elevated levels.
GH-Mediated Lipolysis Mechanisms
During fasting the body undergoes metabolic changes due to increased GH secretion. The primary focus is to maintain levels of glucose for the brain and other glucose dependent tissues like red blood cells. To ensure a supply of glucose the body shifts its preference to using fat as a fuel source preserving stores of glucose and amino acids. Now, let’s talk about muscle. The liver switches to utilizing fat substrates while also releasing glycogen since there is no dietary intake of glucose. In addition large amounts of glucose are released by the liver into the bloodstream to sustain blood sugar levels in the absence of glucose. This process is facilitated by a decrease in serum insulin levels, which prevents released glucose from being taken up by muscle and adipose tissues. Furthermore, elevated GH levels lead to a state of insulin resistance that plays a role in safeguarding reserves of glucose.
The insulin blocking effects caused by GH lower the utilization of glucose. As a result reduce the requirement for precursors derived from muscle protein reserves. This has the advantage of addressing two issues at once. Some experts have opinions on whether GH itself or the rise in FFAss are mainly responsible for this heightened resistance to insulin. However, further exploration of transport and signaling pathways is necessary to delve into this matter.
So to summarize when fasting the increased secretion of GH helps to release FFAs from cells. It also reduces the uptake of glucose, in tissues by regulating GLUT 1. This leads to increased insulin resistance. Prevents glucose oxidation. Additionally GH plays a role in preserving amino acid stores through both indirect means.
What about GH impact?
The impact of GH on lipolysis is well known although the exact mechanisms are not fully understood. It is believed that GH has effects in this process. Firstly it may reduce the activity of lipoprotein lipase (LPL) in tissue. Secondly it can stimulate hormone lipase (HSL) which is involved in breaking down triglycerides into FFAs and glycerol. HSL is considered an enzyme for lipolysis as it determines its rate. However it's worth noting that not all studies have consistently shown an increase in HSL mRNA levels in adipocytes due to GH. As stated earlier it has been observed that GH can directly affect the reduction of LPL activity, in adipose tissues. However, this effect has not yet been proven in muscle tissues. The significance of this finding for individuals aiming to lose fat is that LPL plays a role in removing acids from the bloodstream and either storing them in fat cells or supplying them to skeletal muscles as a source of energy.
Studies conducted on fat cells have revealed that GH (growth hormone) does not directly stimulate the breakdown of fats. However it does enhance the sensitivity of these cells to catecholamines implying that GH activates lipolysis at a stage after the involvement of beta adrenoceptors and/or G proteins. It is reasonable to speculate that GH may increase the density of beta adrenoceptors which could potentially have implications. Previous studies have shown that there are beta adrenoceptors on fat cells and an acute increase in the number of coupled receptors would heighten sensitivity and ultimately promote lipolysis. Additionally in animal models GH has been found to elevate the expression of β3 receptors in fat cells leading to the activation of HSL (hormone sensitive lipase). Therefore apart from its effects, on lipolysis it is logical to assume that using a beta agonist could potentially synergize with GH and further enhance the fat burning process.
Maximum Lipolysis Rate
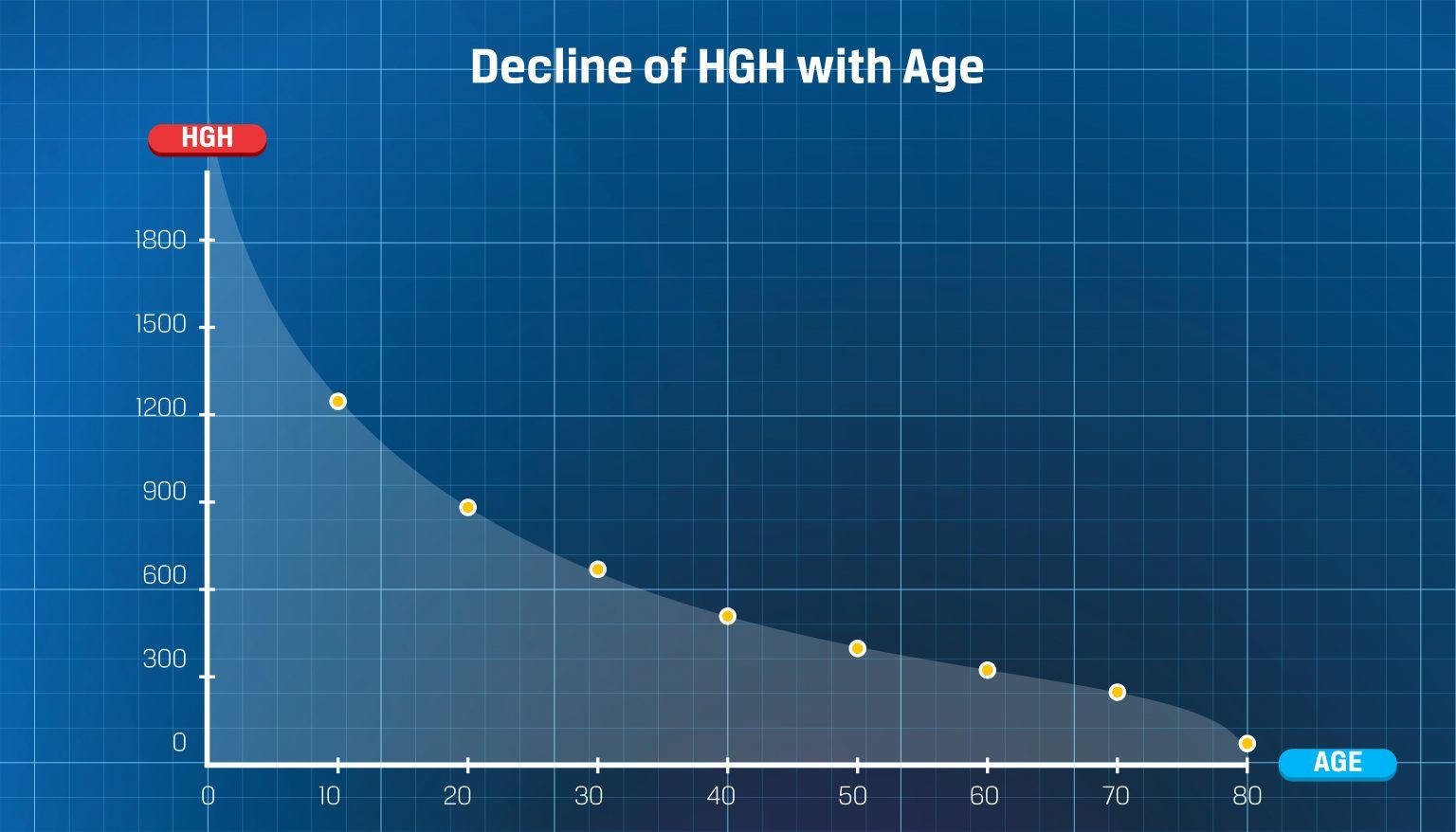
As we strive to develop a combination that optimizes the potential, for fat breakdown is there a cap on how it can happen? Fortunately, we do have an answer, at least in terms of the rate at which intravenously administered GH can trigger the process of breaking down fats. The dosage was determined to be 3 micrograms per kilogram (to an average peak growth hormone concentration of 32.4 micrograms per liter). The dosage does not depend on age or gender. Is approximately equivalent to 1.2 1.5 International Units (IUs) for a lean male weighing 100kg. Taking a dosage does not result in an impact on fat breakdown. Interestingly this dosage aligns with the limit of occurring bursts of secretory activity within the body. It is speculated that this limitation may be due at least in part to how the body clears the substance outside of the kidneys along with levels of circulating growth hormone binding protein (GHBP).
There is some evidence suggesting that this limitation specifically applies to growth hormone (GH) and when it is combined with variations of catecholamines (a type of hormone) there is an effect on breakdown that exceeds what each treatment alone can achieve. This supports the idea that GH plays a role as a mediator in fat breakdown. Some have referred to this as having an effect on catecholamine induced fat breakdown. Anecdotally it appears that combining GH with compounds that stimulate catecholamine production enhances their effects when used together.
Pharmacokinetics and Pharmacodynamics
Understanding pharmacokinetics involves studying how a substance travels through the body, including processes, like absorption, distribution and excretion. On the other hand, pharmacodynamics focuses on the effects that substance has on the body. It is crucial to have an understanding of both concepts when it comes to GH (growth hormone) to fully harness its potential and ensure optimal administration. By doing so we can avoid protocol designs and make the most of our investment in acquiring GH, which can be quite costly. Let's strive not to squander this resource.
Different administration routes have an impact on the pharmacokinetics of Growth Hormone (GH). As we discussed earlier the natural secretion of GH occurs in a manner and the body's negative feedback mechanisms quickly eliminate it from the bloodstream. To closely replicate this secretion pattern one would need to administer GH every 2-3 hours, which's the time it takes for the ultra short feedback (GHRH inhibiting its own secretion) to clear. However I do not. Support this unless under supervision. Instead this article will focus on the two used methods of GH administration; subcutaneous (SC) and intramuscular (IM).
The data presented in this study revealed a finding regarding how males responded to IM versus SC dosing. Despite receiving doses as the SC group, male subjects in the IM group experienced higher peaks of GH release. Actually the group of males receiving IM injections reached the peak as the SC group received higher doses of GH even though they received less than half the amount. On the side the SC group experienced periods of elevated serum GH levels, which has been observed in previous studies as well. This data is fascinating, however there have been trials that show timelines for lipolysis regardless of whether GH's administered through IM or SC injections.
After receiving either SC or IM injections of GH there is a delay before plasma FFA and glycerol levels increase, with fat mobilization peaking around 150-160 minutes. Another important point to consider is the timing of GH injection. Fasting not leads to an increase in natural GH secretion as mentioned earlier but also enhances the responsiveness to exogenous GH administration for fat breakdown. In fact when administered in a state compared to a meal state all markers of fat breakdown are improved. Additionally, remaining in a state leads to an overall clearance rate. It's also worth noting that evening administration of GH has shown bioavailability in growth hormone GHD) individuals. This could be because it closely resembles the occurring evening release of GH although this is mostly speculative, at this stage.

Compound Synergies
When creating a combination of supplements, for fat loss it's important to select compounds that have the potential to work well together and enhance each other's effects.The ways in which GH brings about its effects are complex. Can be understood at a high level. One important pathway involves the beta receptors. It seems reasonable to assume that if we enhance the sensitivity and/or expression of these beta pathways we can further optimize the response to our stack in terms of breakdown. Androgens also have effects by acting on androgen receptors found in adipose tissues. This is interesting because it operates through a pathway than GH. However it has been observed that androgens can increase the expression of beta receptors. As mentioned earlier, increasing the number of coupled receptors in cells can enhance sensitivity. Ultimately boost lipolytic potential. This creates a synergy in our approach to designing stacks.
The relationship between the axis and the GH/IGF axis is fascinating yet intricate. When designing a stack for lipolysis one aspect worth considering is how these axes influence beta adrenergic receptor mRNA levels, their impact on expression – a crucial step in GH mediated fat breakdown. Additionally thyroid hormones stimulate the synthesis, degradation and mobilization of lipids leading to increased levels of circulating fatty acids (FFAs). Another noteworthy characteristic shared by thyroid hormones and GH is their ability to regulate how metabolic processes respond to catecholamines. Once you've achieved a sensitivity and density of beta receptors it only makes sense that utilizing a beta adrenergic agonist would be the perfect addition to fully optimize the potential for fat mobilization.
Practical Applications and Sample Design
Now that we have covered the background information let's discuss how to design a hormone stack and administer it. Also it is important to note that when taking GH it is advisable to do while in a state. While the burning effects of rHGH are not completely diminished by food intake (unlike GH) it would be unwise not to follow this guideline.
Following the fasting recommendations and aiming for a burning response a single injection of 2IU GH would be appropriate. Administering this dose upon waking up in the morning would work well since you are likely already in a state. Subcutaneous injections have a clearance time making them suitable for this purpose especially if you plan on remaining fasted for hours after the injection. To potentially enhance fat mobilization rates further engaging in activity such as LISS or resistance training during this fasting period could be considered. Continuing with the guidelines it may be possible to administer a 2IU injection of GH before going to bed provided that all meals were consumed within a condensed time frame and you enter the evening hours in a partially fasted state.
As mentioned earlier in the article there is evidence suggesting that administering medication, through injections, in the evening may result in increased bioavailability.
To wrap up
If you have to choose between morning (AM) or evening (PM) I would recommend the time mentioned. However if you have the flexibility using a 2IU injection strategy both, in the morning and evening may optimize your body's ability to burn fat over a day as long as you follow the fasting guidelines. By following this growth hormone (GH) dosing protocol along with an androgen stack you can enhance the potential for loss. It is worth considering using anabolic androgenic steroids (AAS) for this purpose and to prevent any risk of muscle loss during periods of calorie deficit. The specific type of androgens used may result in variations in fat loss rates. That goes beyond what we'll discuss here. Even a simple AAS stack based on testosterone would be effective.
To further maximize the potential for burning fat, adding thyroid hormones and clenbuterol to the stack is recommended. These substances work synergistically with androgens and GH as explained in the article. Clenbuterol can be taken once per day due to its properties as can T4. If using T3 it is better to take two doses per day spaced out by 12 hours.
Write a comment